Barrier-busting Approaches to Patient Recruitment
Article
Patient Engagement & Recruitment


Key takeaways from our three-webinar series on patient recruitment:
Today’s patient recruitment environment presents unique challenges that traditional recruitment tactics alone cannot meet. Citeline recently hosted a three-webinar series offering tips to help overcome these roadblocks and lead to smarter, more successful patient recruitment.
The series explores how patient education and trust drive participation, how data and technology can power more tailored recruitment strategies, and how to scale success through real-time patient identification and consistent enrollment support.
In “From Cautious to Committed: How Patient Education & Engagement Drive Trial Participation,” Carley McCobb, Associate Director, Patient Engagement & Recruitment at Citeline, said there are many reasons a patient may hesitate to participate in a clinical trial despite the promise of an innovative therapy.
“We hear fears of side effects, worries about being ‘guinea pigs’ in the industry, and the confusion about what participation actually looks like,” McCobb said. “Then you add in some practical barriers like the distance to the nearest site, the time commitment it might take, or even confusing eligibility criteria, and it’s really no surprise that enrollment suffers.”
Will Franco, Senior Solution Consultant for Patient Engagement & Recruitment at Citeline, said this is where education comes in. “When patients understand the purpose of a trial, what safeguards are in place, and how participation may benefit them and others, they feel empowered,” Franco said.
As part of this education, Franco notes the importance for sponsors “to have a website available for patients and PCPs [primary care physicians] that is tailored around clinical research education” that is inclusive and easy to understand.
Underlining that importance, according to the 2025 Perceptions & Insights study by the Center for Information and Study on Clinical Research Participation (CISCRP), 39% of those surveyed said they would prefer to learn about a clinical research study online.1
McCobb said sponsors are increasingly enhancing trial portfolio websites by adding patient-friendly content that goes beyond listing studies from ClinicalTrials.gov.
She adds that the patient advisors often expressed reluctance to provide their personal data up front unless they know they’re a match for the trial. Adding features such as direct “see if you qualify” call-to-action buttons and pre-screeners enables patients to quickly assess eligibility before sharing that information.
Another trend among sponsors, McCobb said, is to provide disease-specific education pages that serve as a comprehensive resource for patient-friendly materials with relevant imagery and videos. These pages can streamline the search process and improve search engine optimization (SEO), making it easier for patients to find relevant trials online.
Some sponsors also include patient and HCP community portals on their websites. “[These portals] really allow a safe and informative environment where patients, caregivers, healthcare professionals, all of the above can access educational content, discover trials that are relevant to them, and engage with credible resources,” McCobb said. “This also gives sponsors opportunities to reach out to those certain demographic groups or certain healthcare providers to engage with them … to keep those community members informed.”
The takeaway from all this, Franco said, “is that patient enrollment is not just about identifying eligible patients. It’s about helping the patients feel informed, respected, supported during this process.” Staying transparent throughout the recruitment process helps build trust with patients and can turn interest into action.
In “Built-In Data Advantage: Integrating Data & Feasibility for a Tailored Recruitment Strategy,” Lindsay Stahl, VP, Global Head of Patient Engagement & Recruitment, cited four key barriers to recruitment success:
Matt Holms, VP Sales, Patient Engagement & Recruitment, said recruitment challenges largely persist because protocols often become overly complex with eligibility criteria that are difficult, if not impossible, to meet.
“We hear this a lot in talking to different sponsors where the same kind of pieces to the puzzle are at play in … protocols that ultimately look beautiful on paper, but are incredibly hard to execute,” Holms said. “And it starts with a lot of overly complex endpoints. There are a lot of eligibility bottlenecks.
Stahl said traditional feasibility methods rely on fragmented data and historic anecdotal experience, which fail to meet the complexities of today’s clinical landscape. “Too often teams have siloed pieces of information that they need to manually bring together,” she said. “This leads to unpredictable outcomes, and those unpredictable outcomes lead to missed opportunities.”
In addition, Stahl said, protocols often target “unicorn” patients who do not exist in clinical settings, and overburdened sites frequently fail to meet enrollment commitments. Meanwhile, most US healthcare providers (HCPs) are not investigators but have access to untapped patient populations. The question, Stahl said, is how to access those patient populations. Citeline’s approach to feasibility incorporates high-quality proprietary assets with longitudinal real-world data. This combination of holistic, comprehensive data with additional recommendations surfaced by AI uncovers hidden relationships between drugs and between trials and sites, and delivers precise recommendations tailored to a sponsor’s protocol and patient population, Stahl said.
“Looking ahead, especially for small biotechs, [feasibility] will become even more predictive, automated, and integrated,” Stahl said. “We expect in the next three to five years feasibility to be embedded directly into protocol design tools. This is powered by real-time data refreshes and AI-driven simulations so we can model trial scenarios instantly adjusting inclusion criteria, exclusion criteria, a mix of different sites and recruitment strategies basically on the fly.”
For lean teams with limited resources, Stahl said, this means faster decisions, smarter site selection, more confident planning, and reduced operational burden. “So, feasibility doesn’t just need to be a planning exercise, it will be about actually coming forward with an outcome, something that’s pre-engineered,” she said.
In the first generation of patient recruitment, sponsors assumed that 100% of their study would be recruited by the sites they hired, using the patients in the sites’ own databases, said Holms in “The 3rd Generation of Patient Recruitment: Citeline Proprietary Data + RWD + Last Mile Ecosystem.”
“Now this can still be very effective in certain niche indications as well as smaller phases,” he said. “However, the realities of today’s environment present a much more complex, challenging situation to depend just on those sites alone.”
Holms notes that trials are longer than they used to be, and the majority need at least one significant amendment, “which obviously impacts time and planning and money.” There is continual competition for the best sites and often endless change orders to add new sites after the sponsor has already picked the best sites, he adds.
The second generation of patient recruitment, Holms said, became more mainstream about 15 to 20 years ago. “That’s the concept of doing what I would call traditional direct-to-patient advertising campaigns … where you hire a recruitment company to do outreach. They’ll use a variety of different tactics — it could be radio, TV, print ads, newspaper — using proprietary databases that they have to try to target patients within geographic proximity of a site.
“Those patients then have the opportunity to respond through any of those … different outreach tactics and then can opt in to go through an IRB-approved prescreener. All those questions need to be IRB-approved, and they typically are anywhere from seven to 10 questions that cover the protocol criteria. And after they pass those questions, they are then referred and passed on to the site.”
This type of recruitment campaign works well for chronic indications, Holms said. However, sponsors generally do not deploy this strategy right out of the gate. “They’ll pick their sites, and then if those sites aren’t performing, often they will add new sites. Only then do they move to … rescue and bring a recruitment company in.”
Part of the challenge with traditional direct-to-patient tactics, Holms said, is that “they’re not as effective at scale when you get into more complex protocols, when you have IE [inclusion/exclusion] criteria that is labs, biomarkers, gene mutations, specific procedures.” In fact, Holms said, the majority of indications fall into this complex bucket — even some chronic indications like COPD, back pain, and diabetes.
When it comes to putting patients through a prescreening questionnaire, the more questions they can answer, the more qualified they’re going to be when they’re referred to the site, Holms said. “The reality of today’s environment is that the protocols are super-complex, and there’s a lot of critical IE criteria that typically a patient would not be able to self-report.”
Another challenge, he said, is the lack of renumeration for the effort sites have to put in to process these external referrals, which can add further burden to an already overwhelmed site. This is where the third generation of patient recruitment comes in. Holms described this generation as using data to qualify patients well in advance.
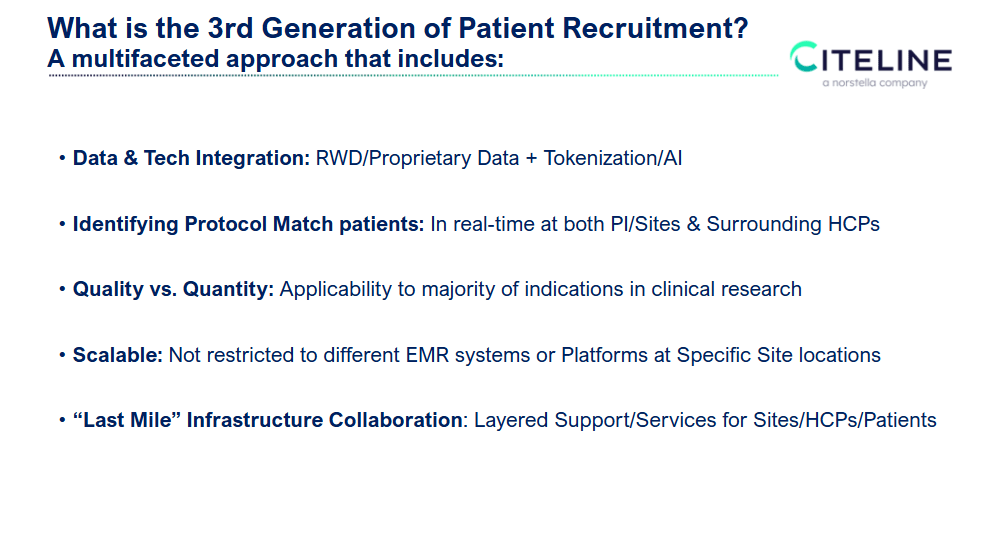
“Citeline PatientMatch is Citeline’s offering that delves into what I’m going to describe as our third generation,” he said. “It’s really a multifaceted approach, and at the heart of it the foundation is data and tech. It’s not just claims data, it’s not just EMR data, it’s not just lab data. Those all fall under the umbrella of RWD, but it’s also Citeline’s proprietary data as well as tokenization … and AI. So, there is a lot of complexity that goes into this approach versus direct-to-patient advertising.”
Citeline PatientMatch also identifies protocol-matching patients in a window of time, Holms said — not just at the sites hired by the sponsors but at surrounding healthcare practices that could be among the 96% not actively involved in clinical research.
“Quality versus quantity … quality in the respect that we’re qualifying these patients based on the protocol and the data before they’re even alerted to the site as well as the applicability to the majority of indications.”
1. Why is patient recruitment so challenging today?
Patient recruitment faces hurdles such as trial hesitancy, complex eligibility criteria, and logistical barriers like travel distance and time commitment. Patients often fear side effects, worry about being “guinea pigs,” or lack clarity on what participation entails. These factors contribute to low enrollment rates.
2. What role does data integration play in recruitment success?
Integrating real-world data (RWD) and feasibility tools helps sponsors predict recruitment outcomes, streamline site selection, and reduce operational delays. AI-driven simulations and real-time data refreshes enable dynamic adjustments to inclusion/exclusion criteria and recruitment strategies.
3. What is the “third generation” of patient recruitment?
The third generation moves beyond traditional site-based and direct-to-patient advertising. It leverages proprietary data, RWD, tokenization, and AI to identify protocol-matching patients across a broader ecosystem, including healthcare practices not actively involved in research.
1 Center for Information and Study on Clinical Research Participation (CISCRP) 2025 Perceptions and Insights Study. Available from https://www.ciscrp.org/professional-services/perceptions-and-insights-studies [Accessed Nov. 14, 2025]
To enable the booking feature, please enable all cookies in your browser.





