Retired Researcher Puts the (Mis)use of Race in Medicine Under the Microscope
Article
Clinical

Physicians must use care in applying group-level assumptions or stereotypes onto individuals, particularly in clinical trials. Retired researcher Ted Marcy encourages a paradigm shift.
“The incidence of disease,” said retired physician Ted Marcy, “is not Black and white.” His presentation, “Misuse of ‘Race’ in Medicine, Redefining What Health Equity Means,” was part of an online speaker series sponsored by A Long Talk. He was introduced by Kamal Carter, president of the organization that was inspired by the death of George Floyd.

Marcy was a pulmonary and critical care physician and emeritus professor of medicine at the University of Vermont (UVM). He chaired UVM's human research ethics committee in behavioral and social sciences, also known as an institutional review board (IRB). The board was reviewing whether protocols involving human research participants were adhering to federal regulations on human research.
When he was a practicing physician, Marcy said in his medical notes he would have identified a patient as a 30-year-old Black male bank clerk who presented with a chief complaint of shortness breath for two weeks. “What do I mean by Black? I mean, how did I define that? … Did I measure blackness? … Did I ask them to identify themselves? I generally did not. I sort of did it based on appearance.”
Marcy identified himself as someone who previously used a race-based approach to medical care. “Biologically,” he said, “there is only one race within our species of homo sapiens. If you look at DNA samples from humans across the world, you see that there's a continuum of genetic variation, but there's no place where you can draw a line and say there's a major difference on one side of the line from the other.” He maintains that these designations do not generally provide a direct causal explanation for observed health conditions and outcomes.
Instead of being race based, Marcy said “we need to be race conscious when we practice medicine. … So is sickle cell anemia a Black disease?” In people with sickle cell disease, their red blood cells contain mostly abnormal hemoglobin S. This mutation confers a significant survival advantage in areas where malaria is prevalent or endemic. While there is a higher frequency of the hemoglobin S gene in Sub-Saharan Africa, Marcy noted there is also a fairly large amount of hemoglobin S in Greece, the Middle East, and even in the subcontinent of India. Sickle cell diseases are more prevalent among those populations. Conversely, Marcy challenged the widely held belief that cystic fibrosis is a “white” disease.
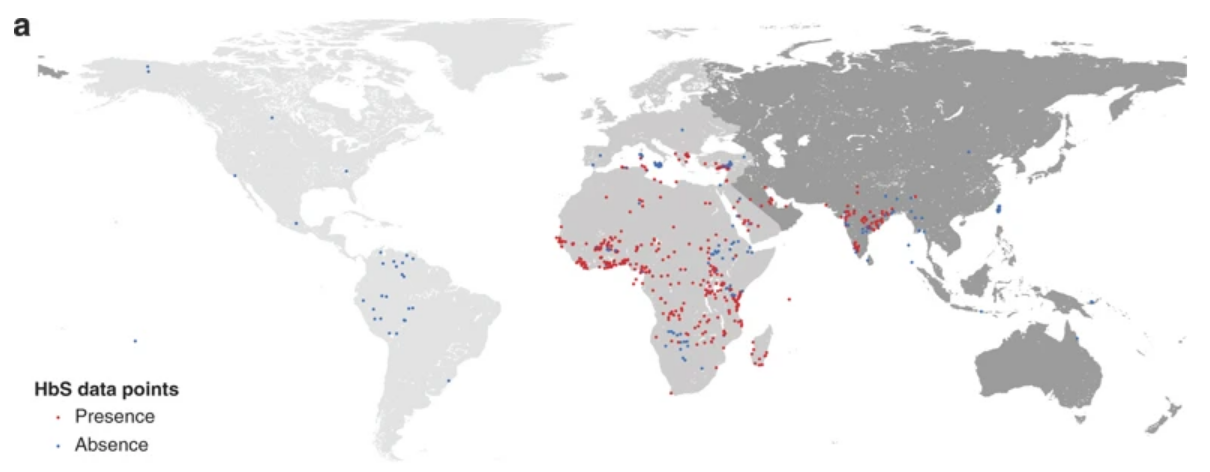
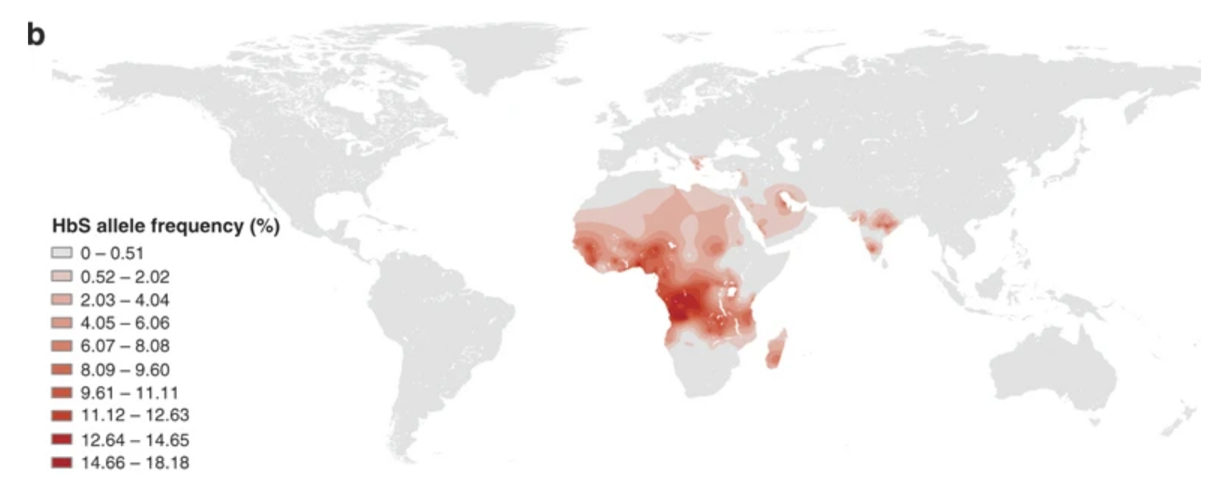
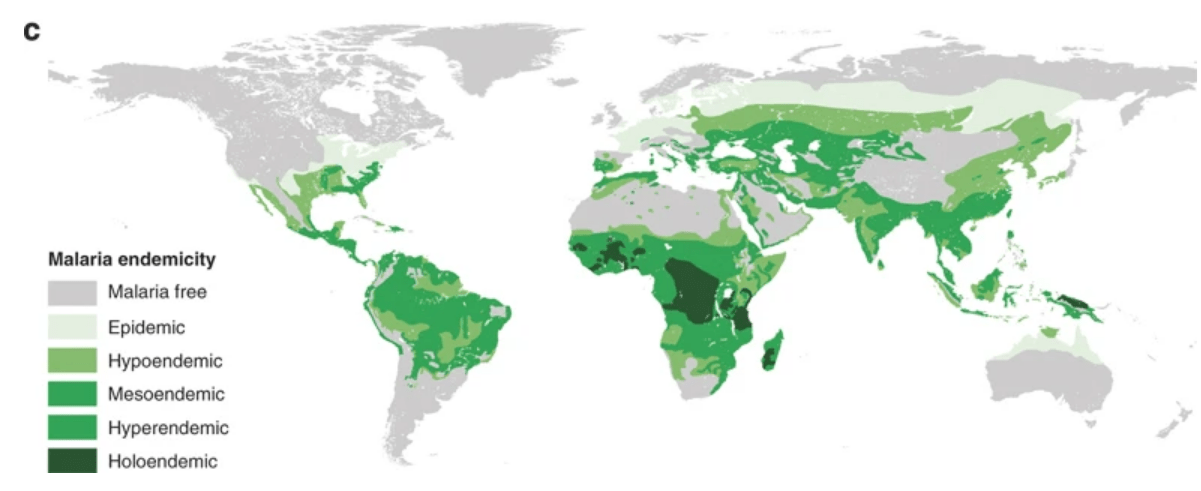
Source: Nature communications1
“So sickle cell diseases is not exclusively a black disease,” Marcy said. “It's more nuanced than that. If you attach an innate biological risk to an individual because of their socially identified race,” it increases the likelihood of a misdiagnosis. Using a race-based approach pathologizes race, he asserted. “Race is a proxy for the real underlying causal factors.”
In discussing prevalence of diabetes, Marcy posited the question: Is this just inherent in being Black or is there a different reason? He cited social determinants of health (SDOH) including socioeconomic status (SES), education, occupational level, and income. “If we look at SES … and the prevalence of diabetes, all comers, you are much more likely to have diabetes if you have less than a high school education, regardless of your identified race,” he said.
Marcy provided other examples of race-based medicine, such as race-based algorithms for medical tests. These include pulmonary function tests with race-corrected “normal” limits and estimates of kidney function (GFR) in Blacks vs. whites.
“As a researcher and member of study section and … also from my IRB experience, there is much more of a requirement now that researchers include individuals of different racial categories.” He said that conducting research in Vermont, with a white population hovering around 95%, that became difficult. But the National Institutes of Health (NIH) encouraged collaboration with researchers in other parts of the country with higher proportions of different races in order to have a diverse cohort with adequate representation.
“So how do we get to a race-conscious approach to medical care?” Marcy asked. He said the first step is to “avoid including race in the chief complaint or medical history narrative and instead elaborate in the social history at a much more granular level.” Referring back to his medical notes, he would have included details such as the patient is a new American who identifies as Black, who immigrated from South Africa after completing college, is employed full-time, married, and owns his own home.
Marcy warned that physicians must use care in applying group-level assumptions or stereotypes onto individuals. “What I witness a lot of times is that in the healthcare industry,” he said, “they lump everybody together. And I think women could probably understand a lot better, right? In that the research only seems to be based on white men.” He mentioned that a number of articles in The New England Journal of Medicine have highlighted the need to become race conscious as opposed to race based or even race blind.
“Race and ethnicity are social constructs,” he said.
Learn how Global Patient Insights uses RWD and SDOH to help sponsors identify geographical areas with underrepresented patients and help determine pockets of patients with unmet needs.
1. Are conditions like sickle cell anemia or cystic fibrosis tied to specific races?
According to retired physician Ted Marcy, no. Sickle cell anemia is often mislabeled a “Black” disease, but the gene responsible for it is found in populations from regions historically affected by malaria. Likewise, cystic fibrosis is incorrectly stereotyped as a “white” disease. These conditions are tied to ancestry and geography, not socially defined race categories.
2. What role do social determinants of health play in disease prevalence?
Marcy highlights that factors such as socioeconomic status, education, occupation, and income have a stronger influence on disease prevalence than race. For example, individuals with less than a high school education have a higher likelihood of developing diabetes, regardless of their race.
3. How can clinicians adopt a race-conscious (rather than race-based) approach to healthcare?
Marcy recommends removing race from the chief complaint or medical history and replacing it with more detailed social and environmental context. For example, instead of labeling a patient as a “30-year-old Black male,” physicians should note relevant factors such as immigration history, socioeconomic situation, or community context. The goal is to focus on real health determinants rather than assumptions associated with racial categories.
1Piel, F., Patil, A., Howes, R. et al. (2010) Global distribution of the sickle cell gene and geographical confirmation of the malaria hypothesis. Nat Commun. Available from: https://doi.org/10.1038/ncomms1104
To enable the booking feature, please enable all cookies in your browser.





