Tracking Diversity in Clinical Trials: The Challenge of Consistency
Article
Clinical

Many challenges impede the implementation of diversity in clinical trials. One that sometimes flies under the radar is the lack of data to track the trajectory of clinical trial diversity reporting.
Johns Hopkins conducted a study in 2022 that examined the reporting of racial, ethnic, and gender demographics in 27 bladder cancer trials published from 1994 to 2021 that enrolled nearly 1,700 patients. It then compared these data with the rate of new bladder cancer cases and deaths.1
All the trials included data on patient gender, but only 40% had any data on patient race or ethnicity. And of those that did report, 94% of the participants were white, 2.1% were Black, and 0.6% were Hispanic. “Black and Hispanic patients were significantly underrepresented relative to their proportion of new bladder cancer cases and deaths,” says Johns Hopkins urologist Max Kates, M.D.1 A related collaborative study that reviewed 514 clinical trials conducted between 1970 and 2020 found that only 24 of those studies — 4.4% — reported racial demographic data. Of those enrolled in the 24 studies, between 2% and 8% were African American, and between 2% and 5% were Hispanic.1
A related collaborative study that reviewed 514 clinical trials conducted between 1970 and 2020 found that only 24 of those studies — 4.4% — reported racial demographic data. Of those enrolled in the 24 studies, between 2% and 8% were African American, and between 2% and 5% were Hispanic.1
The US Food and Drug Administration (FDA) is working to change the lack of reporting around diversity. In 2016, the FDA put out a guidance document on the collection of race and ethnicity data in clinical trials. In it, the agency recommends five classifications for race and a two-question format for Hispanic ethnicity. It also recommends use of more detailed racial and ethnic categories for trials conducted outside the US.
But therein lies a problem. Not having one standard for racial and ethnic data reporting can result in data discrepancies across the board. And often the electronic patient databases sponsors rely upon to obtain data on potential clinical trial patients are sorely lacking in consistent, reliable data on race and ethnicity.
 Ubong Peters
Ubong Peters
In a recent Citeline webinar, “Diversity in Clinical Trials: Data, Disclosure, and Due Diligence,” panelists discussed these discrepancies and what can be done about them. Ubong Peters, lead clinical scientist at Genentech, a member of the Roche group, says one of the biggest challenges faced by diversity efforts is the standardization — or lack thereof — of reporting of race and ethnicity in clinical trials.
“When you’re reporting [diversity] to ClinicalTrials.gov or in the clinical trials files that we have been conducting as industry, there tends to be a lack of standardization of that process,” Peters says. “In some instances, the sites or whoever is acquiring that record is using the self-report of the patient. And then in other cases, whoever’s making that record is actually just looking at the patient and based on how they look, they enter that record. That is one very big problem because now there is a disparity between real-world data that you get from electronic health records or from other data sources like the medical claims and so on, versus data that you are getting from clinical trials. It’s a little bit disjointed.”
Without addressing this problem, Peters says, it will be hard to say whether the industry is making progress in making clinical trials more diverse.
“If you ask me now, what is the percentage of Black or African American patients with multiple myeloma, and if I were to look at a number of the data sources that we have, they will all report different numbers,” he says. “Some could say it’s 25%, others would say it’s 30%, another would say it’s 15%. Which one is the right one? And now that the FDA is calling us to have these diversity targets, this is going to be an important question to address for us to really be able to start tackling that.”
 Nader Daoud
Nader Daoud
Nader Daoud, senior manager, clinical trial diversity & inclusion, patient and site experience (PASE) at Moderna, says he believes that self-reporting is the way to go for race and ethnicity.
“There are social constructs. You can’t judge someone by the way they look and be able to ascertain that,” he says. “But there’s also this extra layer of complexity when talking to people is that we talk about race and ethnicity, which are again, social constructs in a very US-centric way. We ask people if they're Black or African American or native Hawaiian or other Pacific Islander. If you're Samoan, I'm sure that doesn't feel great. Or you might be in Britain and think, well, I’m Black or African British.”
Daoud notes that both the US Centers for Disease Control and Prevention (CDC) and the Clinical Data Interchange Standards Consortium (CDISC) are expanding their standard lists of racial and ethnic categories, including in the CDC’s case-specific American Indian and Alaskan native tribes.
“How do you incorporate that in order to be able to give patients the power to select however they identify, but still have statistical power behind when you send your reports to the FDA or other regulatory bodies?” he asks. “That’s part of this diversity plan guidance that they’re releasing. A lot of the questions that I’m sure other sponsors have also asked is, ‘How do you see us navigating this space?’ You can’t go to a global area in a global trial and ask people US-centric questions. That’s not how race and ethnicity work.”
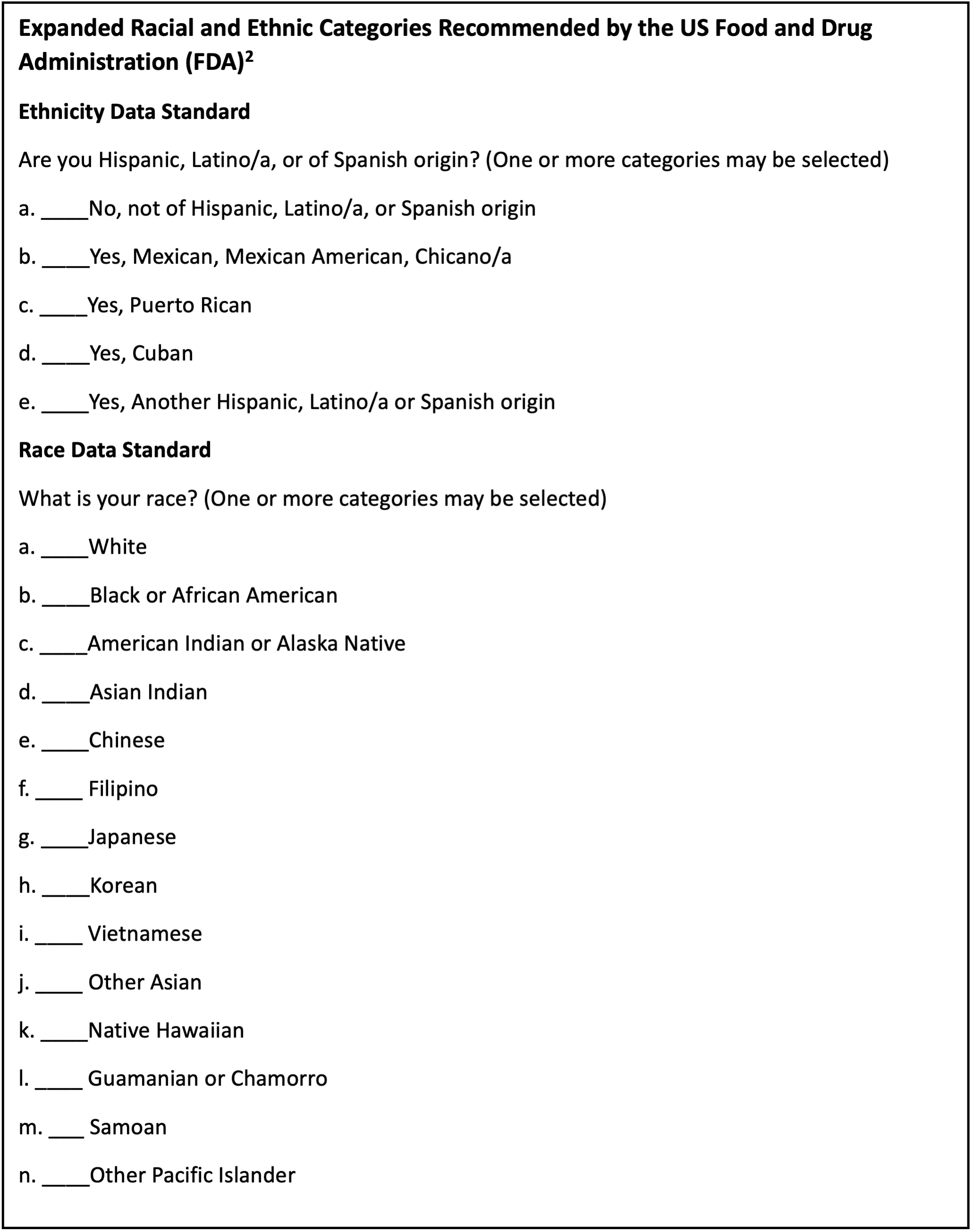 Source: US Food and Drug Administration (2016) Collection of Race and Ethnicity Data in Clinical Trials. Available from https://www.fda.gov/media/75453/download [Accessed Oct. 11, 2023].
Source: US Food and Drug Administration (2016) Collection of Race and Ethnicity Data in Clinical Trials. Available from https://www.fda.gov/media/75453/download [Accessed Oct. 11, 2023].
Daoud says there are ongoing conversations around artificial intelligence (AI) and other platforms that are pulling lots of information together.
"Big data is everywhere,” he says. “But what does that data look like? Where are you pulling it from? Who got asked those questions? When you look at censuses, are the governments that are doing them equitable governments? Are they trying to hide certain populations that are ethnic minorities or otherwise? It’s very sensitive. Do they even collect race and ethnicity in the EU? There are certain countries in the EU where you can’t even ask someone what they identify as racially, ethnically. You need to ask something like, what’s your socioeconomic background. And then they understand what you’re asking.”
Daoud says he believes it’s a question of how the industry thinks about operationalizing this information in clinical trials. “I know it’s popular in everything that I just said to think about the ethical portion last,” he says. “You talk about all the possibilities and then you say, but there’s ethical bias or there’s some sort of bias in the dataset. It’s about acknowledging all that first and taking it into consideration at the very first step.”
When conducting trials globally, Daoud says, “You have to actually see what’s reasonable for that region, what’s actually applicable. So, when we think about using real-world data, we use a bunch. We use claims data, we use census data, we use epidemiological data, surveillance data. We take all that and try to marry it together in order to make sense.”
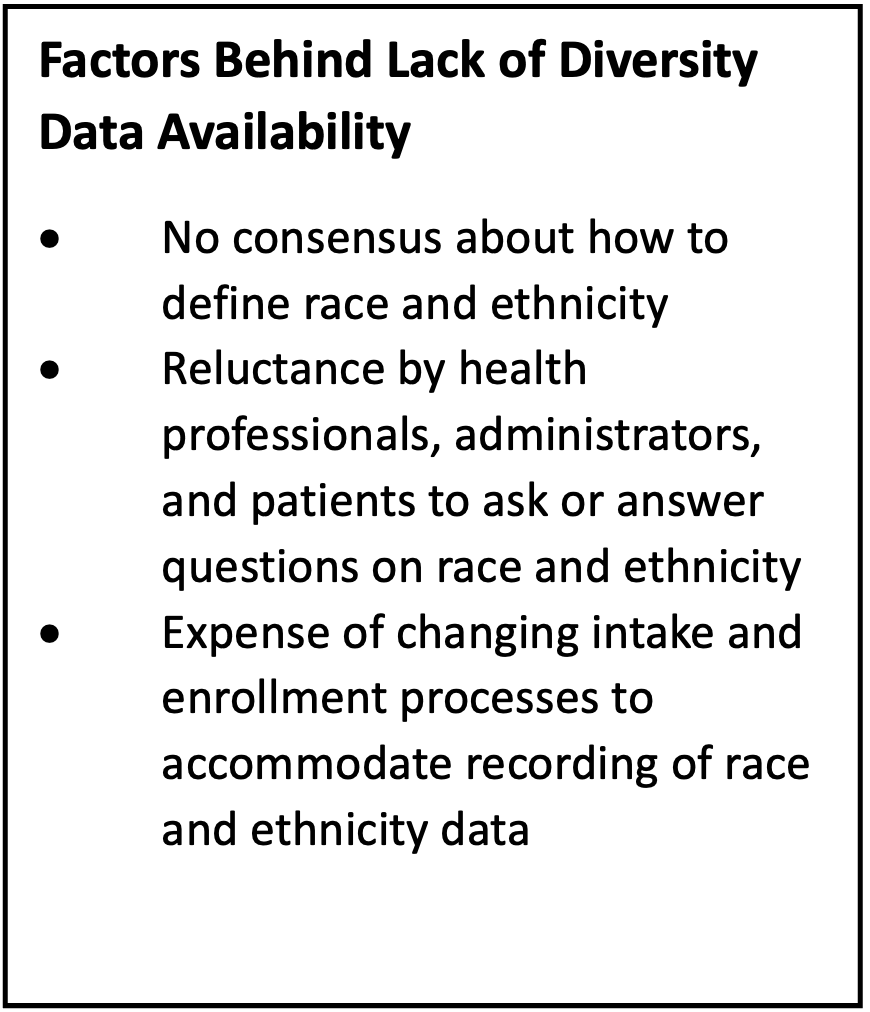 Source: Blumenthal D and James CV (2022) A Data Infrastructure for Clinical Trial Diversity. The New England Journal of Medicine, 386, 2355-2356. Available from https://www.nejm.org/doi/full/10.1056/NEJMp2201433 [Accessed Oct. 11, 2023].
Source: Blumenthal D and James CV (2022) A Data Infrastructure for Clinical Trial Diversity. The New England Journal of Medicine, 386, 2355-2356. Available from https://www.nejm.org/doi/full/10.1056/NEJMp2201433 [Accessed Oct. 11, 2023].
Daoud says Moderna takes all that information and sets scores for each of its sites with regard to demographic objectives for individual study enrollment. “So, we can see historically how they’ve performed against the goals that we’ve set so we can have an idea of sites that might be better in order to recruit a certain population or subpopulation. Again, it's not just the external data or real-world evidence, but the real-world data that we have from our own trials and other trials that have been performed.
“It wasn’t until 2015 that the FDA required drug trial snapshots to actually say what race and ethnicities you enrolled in your trial. So now we have all that, and we have the tools to make it actionable.”
Peters says the key part that concerns him is the lack of standardization across datasets, as well as the fact that the real-world data being relied upon is not clean.
“Data in the real world is all over the place,” he says. “So, when you then use it to guide your site selection or study feasibility decisions, it’s quite likely that you could also be causing more issues around underrepresentation because you’ve relied on a dataset that was quite exclusive in the way it was being collected.”
For instance, Peters says, the data may be based on patients who had an actual diagnosis and were part of the healthcare system in some form or capacity. They may have visited a particular healthcare center that has an electronic health records (EHR) platform, or they may have had insurance. “So, they’re being tracked through the medical claims database in that way,” he says. Then there are patients who receive care in the community, and their safety net community hospitals don’t have EHR platforms, Peters says. Or they do have EHR platforms but they don’t have the IT infrastructure to be able to query and pull some of that data through the inclusion/exclusion criteria of the study to identify potential patients at that location. “At the end of the day, we do have to make a hard choice,” he says.
For instance, Peters says, the data may be based on patients who had an actual diagnosis and were part of the healthcare system in some form or capacity. They may have visited a particular healthcare center that has an electronic health records (EHR) platform, or they may have had insurance. “So, they’re being tracked through the medical claims database in that way,” he says.
Then there are patients who receive care in the community, and their safety net community hospitals don’t have EHR platforms, Peters says. Or they do have EHR platforms but they don’t have the IT infrastructure to be able to query and pull some of that data through the inclusion/exclusion criteria of the study to identify potential patients at that location.
“At the end of the day, we do have to make a hard choice,” he says. “Yes, any data is better than no data at all, but we still have to deal with it with a grain of salt, understanding that the data just doesn’t give us a full picture. We have to rely on other ways of generating insights for now at least until such a time when we have built a more robust data infrastructure. And we badly, badly need to have this kind of infrastructure in place.”
 Chrissa McFarlane
Chrissa McFarlane
“There really exists today no central source of truth for information,” says Chrissa McFarlane, founder and CEO of Patientory.
“You’re getting data from EMRs, from censuses, from community organizations…. There’s really no one tracking system or, I would say, quality metrics to also enforce this, but also have that transparency. And once we step in the right direction of being able to monitor and really track that, then we can start to see more of these diversity hurdles and challenges that we’re addressing in the system both nationally and internationally, because healthcare exists differently outside the US, where they take a more top-down approach, than here, which is more fragmented.”
1 Johns Hopkins Medicine (2022) Race, Ethnicity and Clinical Trials. Available from https://www.hopkinsmedicine.org/news/articles/2022/11/race-ethnicity-and-clinical-trials [Accessed Oct. 11, 2023].



A biotech need to rapidly meet diversity/inclusion goals for a high-profile Phase III COVID-19 trial. Citeline Connect helped the sponsor recover from a 72% decline in diversity-focused randomizations, delivering 20-25% of daily randomizations in 32 days.
To enable the booking feature, please enable all cookies in your browser.

