An Alphabet Soup of 2026 Predictions: GLP-1s, ICH, GCP, CAR-T, AI & More
Article
Clinical

Our annual predictions article covers it all — from clinical planning to patient recruitment to clinical trial disclosure. See what Citeline and industry experts have to say on where pharma is headed for 2026.
Thought leaders in every industry are making their predictions as to how 2026 will pan out, and the life sciences is no exception. Read on for forward-looking insights into clinical planning, patient recruitment, clinical trial disclosure, and more.
 Izabela Chmielewska
Managing Editor,
Custom Content
Citeline
Izabela Chmielewska
Managing Editor,
Custom Content
Citeline
 Andrew Warmington
Manufacturing Editor
Citeline
Andrew Warmington
Manufacturing Editor
Citeline
Throughout the industry, there is a clear push for earlier and cleaner evidence, says Izabela Chmielewska, Citeline Managing Editor, Custom Content. Teams want to make confident decisions sooner, she says, which is driving tighter study designs and a stronger focus on what can be learned in the first stages of development.
In addition, she says community-based research is moving from small pilots to something sponsors are willing to build into their core strategy. The priority now is proving that it strengthens timelines, retention, and data quality in a reliable way.
Controlled models also are gaining attention, Chmielewska notes, because they offer clarity at a point where field trials can be unpredictable. They help teams refine programs before they commit to larger, more expensive studies.
Another trend Chmielewska sees is that trial design is becoming more pragmatic. Sponsors are thinking more carefully about what is realistic for patients and what supports sites, and that shift tends to produce smoother studies with clearer data.
Citeline Manufacturing Editor Andrew Warmington predicts contract development and manufacturing organizations (CDMOs) will become more focused on long-term partnership and full-service offerings, with increased investment in novel modalities. He adds that small molecules should remain dominant as first-line treatments.
 Matt Holms
VP of Sales
PE&R
Citeline
Matt Holms
VP of Sales
PE&R
Citeline
Matt Holms, Citeline VP of Sales for Patient Engagement & Recruitment, sees a couple of major trends taking hold in 2026. First, sponsors will leverage both data and AI for comprehensive patient matching. More specifically, they will combine real-world data (RWD) and proprietary data with tokenization and AI to locate hard-to-find patients.
Second, he cites the integration of data as “the foundational continuum for feasibility as well as patient recruitment. Successful recruitment doesn't start once the study starts,” he says. “It begins at protocol design/site selection.”
 Jake Mathon
Senior Manager
Citeline
Jake Mathon
Senior Manager
Citeline
“Obesity is definitely having a moment,” says Citeline Senior Manager Jake Mathon. Yearly new industry trial starts are up 500% since 2020, a trend he expects to continue. According to data from Citeline's Pharmaprojects, new drugs in development have had steady growth with dramatic increases since 2023 to a total of 567 individual projects. With about half of those drugs still preclinical, he says we can expect to see continued new trial growth.
GLP-1 drugs are all the rage, but Mathon cautions that their success has been limited by side effects and high costs. Any new entrants into the space will need to compete favorably on one or both of these factors as well as offer equal or better efficacy.
Warmington adds: “Obesity/diabetes will become even more dominant as oral GLP-1s are developed and prices fall.”
Mathon notes that the US Food and Drug Administration (FDA) and prescribers will still want to see positive cardiovascular outcomes from trials that are quite large and long, likely negating any advantage to compete on cost. He expects any true GLP-1 competitors to have considerable gains in efficacy with better tolerability.
Median time to approval for obesity drugs from Phase I to new drug application (NDA) or a biologics license application (BLA) is just under seven years. Mathon says drugs just starting Phase I now could be potentially gaining approval just before the first wave of generics for GLP-1s start hitting the US market.
 Heidi Chen
Associate Director,
Research & Commercial Support
Citeline
Heidi Chen
Associate Director,
Research & Commercial Support
Citeline
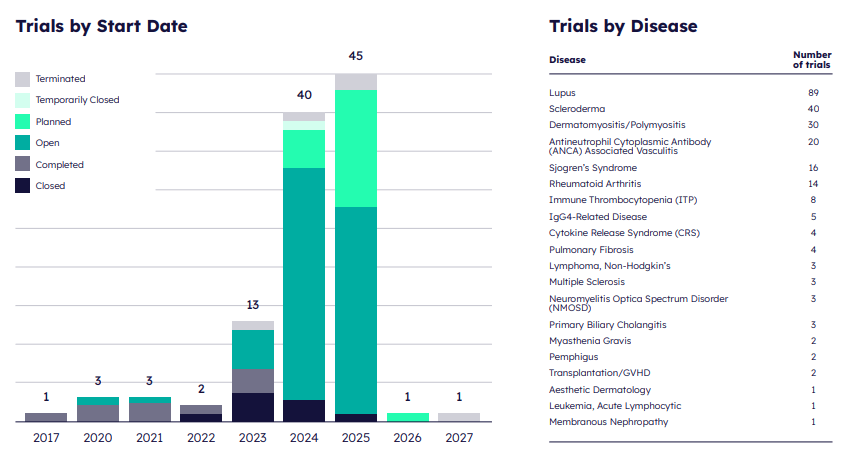
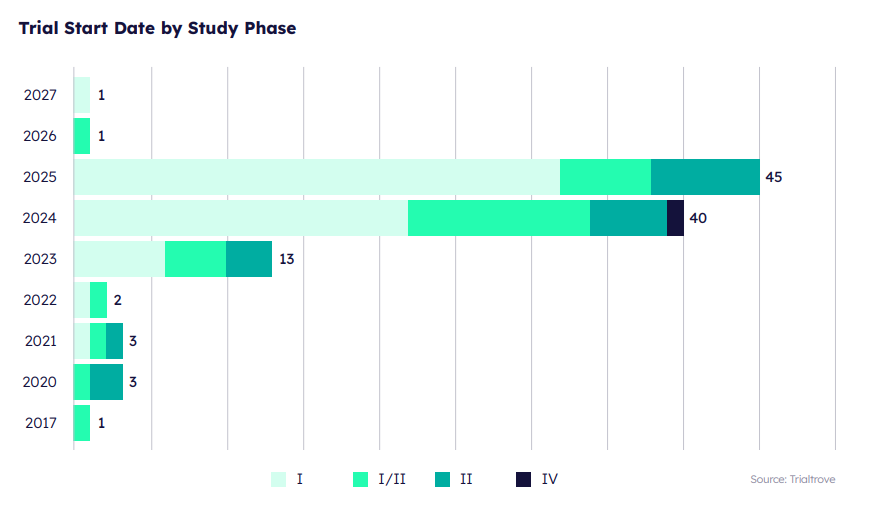
Based on Trialtrove data, it appears likely that the recent upward trend will continue for clinical trials in autoimmune diseases involving chimeric antigen receptor T cell (CAR-T) therapy.
Heidi Chen, Citeline Associate Director, Research & Commercial Support, says, “We wouldn't be seeing lots of trials populating in 2026 and 2027, because these are planned and completed trials. The number of trials will increase as we progress into these years.” She adds that sponsors report trials at a later date, creating a lag in the data.
 Wes Michael
President and Founder
Rare Patient Voice
Wes Michael
President and Founder
Rare Patient Voice
Many of these autoimmune diseases fall into the rare disease category, which is poised for an uptick in research. “In 2026, I'm confident that the number of clinical trials for rare diseases will continue to increase,” says Wes Michael, President and Founder, Rare Patient Voice. “Orphan drugs are now exempt from several negative provisions of the [US] Inflation Reduction Act, and many expect the FDA to be more favorable in regulating rare disease drugs.”
The International Council for Harmonisation (ICH) updated its Good Clinical Practice (GCP) guideline, effective as of July 23, 2025. According to Claire Riches, Citeline VP of Clinical Solutions, the pharmaceutical industry’s overall data and AI strategy actually lines up very closely with what the updated ICH GCP E6(R3) is pushing for: risk-proportionate, data-driven, tech-enabled trials with much stronger data governance and oversight.
 Claire Riches
VP of Clinical Solutions
Citeline
Claire Riches
VP of Clinical Solutions
Citeline
 Francine Lane
Head of Transparency
Citeline
Francine Lane
Head of Transparency
Citeline
 Ben Evans
Disclosure Regulations
Research Manager
Citeline
Ben Evans
Disclosure Regulations
Research Manager
Citeline
Riches says the industry's move to shared data products and integrated platforms in 2026 is essential to meeting these expectations — central data assets and AI services can be governed, validated, and audited more consistently than fragmented local tools.
In short, Riches says, if pharma uses 2026 AI and data investments to strengthen quality by design (QbD), risk-based quality management (RBQM), centralized monitoring, and data governance — rather than to “black box” decisions — those strategies will be highly compatible with, and in many cases enabled by, ICH GCP E6(R3).
Francine Lane, Citeline Head of Transparency, points out that the UK Medicines for Human Use (Clinical Trials) (Amendment) Regulations 2025 goes into effect in April 2026, so that will be a major focus for those conducting trials there. She says these requirements correspond more closely with the Good Clinical Practice guidance and the Declaration of Helsinki than others. “It’s an ethical framework, not just a compliance checkbox,” she says. “I think there will be a broader trend to register and provide summary results for all trials conducted in humans, at least by the time that the product reaches approval.”
Lane says this aligns with what Jennifer Miller and Bioethics International is doing with the Good Pharma Scorecard. “Even when regulations haven't caught up,” she says, “there's growing momentum towards transparency as an ethical imperative. The question of 'Should I register this trial?' is being replaced by 'Yes, of course this trial will be registered.’”
Ben Evans, Citeline Disclosure Regulations Research Manager, predicts that ISRCTN will increasingly become the preferred “go-to” registry for international clinical trials in 2026, potentially overtaking ClinicalTrials.gov in usage outside the US. ISRCTN is a registry following requirements set out by the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) and the International Committee of Medical Journal Editors (ICMJE) guidelines. The US government shutdown had disrupted ClinicalTrials.gov operations, causing registration delays for non-US-required studies, while ISRCTN actively promoted its availability and implemented platform enhancements to accommodate increased submission volumes.
 Kemi Williams
Senior executive in clinical
research & population health
Kemi Williams
Senior executive in clinical
research & population health
Data quality is becoming the real test for new digital and analytical tools, says Citeline's Chmielewska. Regulators want clarity about how data are collected and handled, and sponsors are far more selective about the datasets they choose to rely on.
Kemi Williams, a senior executive in clinical research & population health, says companies will evolve from broad, awareness-style diversity efforts to hyperlocal, data-driven strategies that incorporate social determinants of health, geospatial insights, and real-world evidence to identify where unmet need truly lies. Incomplete or non-representative datasets, she says, undermine confidence among patients, providers, payers, and regulators.
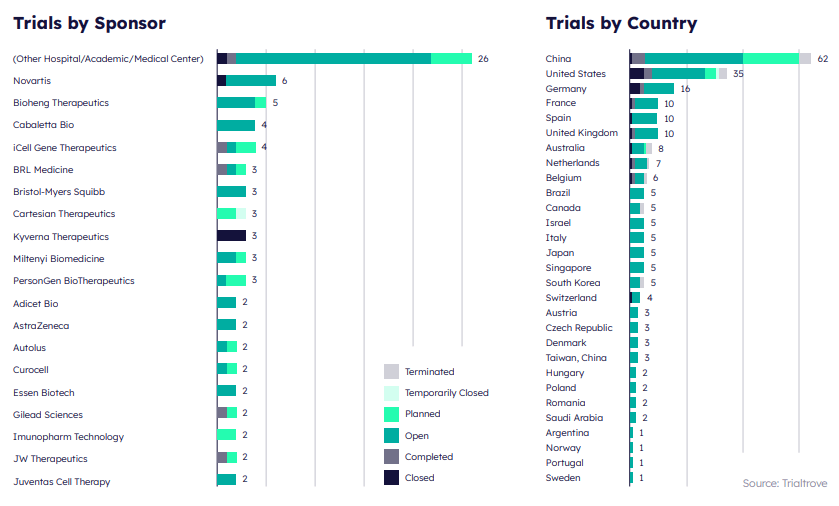
APAC is becoming a central part of global development planning, says Chmielewska. Sponsors see the region as a way to gain speed, secure strong scientific oversight, and benefit from more predictable operations.
More specifically, Chmielewska says China is playing a larger role in global R&D. More programs are being designed with international acceptance in mind, and partnerships between Chinese innovators and Western pharma continue to increase.
“As we move into 2026, clinical trial diversity will shift from a compliance expectation to a commercial and scientific necessity,” says Williams, who has worked for AstraZeneca, Roche, Abbott, and other major players. Biopharma companies, she says, are recognizing that market success increasingly depends on whether medicines demonstrate value across the full spectrum of real-world patients that can benefit from their products. Robust representation strengthens models of safety, efficacy, and long-term adoption.
“Ultimately,” she adds, “ensuring clinical trial representation is becoming a competitive advantage, not just a moral imperative. The companies that win commercially will be those that integrate inclusive research from R&D through commercialization, aligning protocol design, evidence generation, medical affairs, value messaging, and patient engagement under a cohesive population-science strategy.”
No predictions piece, regardless of the industry, would be complete without mentioning artificial intelligence (AI). Data scientists at Norstella, Citeline's parent company, note the use of AI to promote diversity in clinical trials. AI-powered systems, they explain, are used to reduce human bias in trial design and to balance the goal of increasing participant diversity with the need to deliver the trial on time and on budget.
In addition, these experts share that AI-powered recruitment platforms now enable real-time demographic balancing and adaptive enrollment strategies, helping sponsors meet and exceed diversity targets. Edge AI is increasingly being assessed for its potential to support decentralized clinical trials (DCTs), which will improve trial accessibility and retention, especially for underrepresented populations.
According to Open Data Science, the future likely holds even more sophisticated AI applications. Imagine systems that can predict which communities will most likely benefit from a particular treatment or platforms that automatically adjust recruitment strategies in real time to improve diversity.
A recent industry analysis predicts the AI market will grow from $4.35 billion in 2025 to about $25.73 billion by 2030 for the pharmaceutical sector, driven by innovations in drug discovery, clinical trials, precision medicine, and commercial operations. Within that, generative AI is set to expand at a 43.12% CAGR through 2030 (generative AI is set to expand at a 43.12% CAGR through 2030 (Mordor Intelligence).
Citeline's Riches, relating back to ICH GCP E6(R3), says that focusing AI on a small set of high value use cases — such as protocol design, risk assessment, centralized monitoring, and critical-to-quality (CtQ) dashboards — helps sponsors identify, quantify, and continuously manage key risks “instead of generating noise.”
She notes that in 2026 the industry will be making a concerted push towards formal AI governance, AI product owners, and cross-functional data/AI squads. This will make accountability for AI-enabled processes explicit and reviewable.
Riches adds: “Investing in AI agents and analytics for centralized monitoring, outlier detection, and trend analysis is therefore not just permissible but aligned with the guideline's vision, provided validation, documentation, and risk controls are in place.”
Williams predicts AI will increasingly reshape protocol development by identifying exclusionary criteria, predicting enrollment barriers with higher accuracy, and modeling population-level feasibility. Companies using AI-assisted design, she says, will see improved enrollment timelines and more representative patient pools, which can directly strengthen the quality of clinical and commercial evidence.
 Domenique Catalano
Senior Manager
Citeline
Domenique Catalano
Senior Manager
Citeline
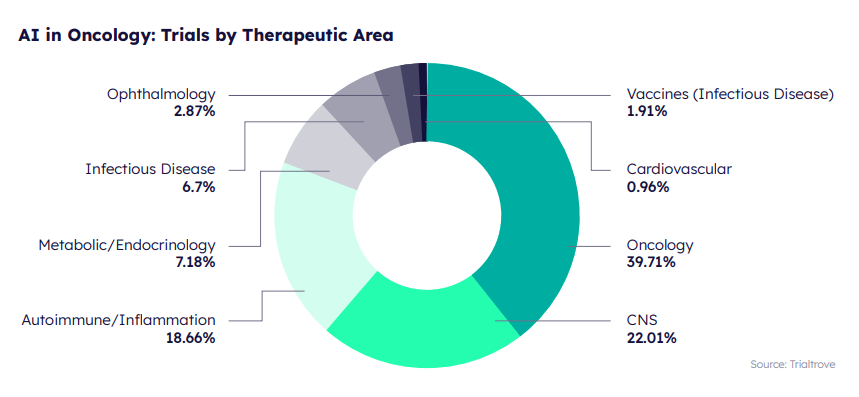
AI and machine learning (ML) models are now gaining momentum in oncology trial design, says Citeline Senior Manager Domenique Catalano. This momentum is driven by adaptive protocols, predictive models for better patient recruitment, stratification and selection, accelerated data analysis — including the use of RWD or electronic health records (EHRs) — and real-time monitoring through decentralized components. She adds that AI and ML elements aid in precision medicine and early cancer detection.
Catalano points out that several AI-driven tools are utilized in oncology trial designs to refine patient selection. For example, Citeline's Protocol SmartDesign utilizes a sophisticated algorithm that leverages ML and large language models (LLMs) to analyze historical trial data, generating an accurate predictive model of successful trials. Citeline's Protocol SmartDesign reduces the time it takes to create protocols by recommending primary endpoints and inclusion/ exclusion criteria, giving medical and clinical operations teams a head start on protocol development.
Moving into 2026, Catalano says, “AI and ML will continue to help reshape how we understand and treat cancer, potentially revolutionizing trial design and patient outcomes.”
In the regulatory realm, Citeline's Evans predicts that AI-powered tools for intelligent content parsing, automated document analysis, and multilingual translation will become increasingly adopted by registries globally, streamlining registration workflows and reducing manual data entry burdens for researchers.
“AI is obviously going to have a big impact on disclosure and regulatory,” Citeline's Lane says. “Sponsors and vendors are all experimenting with AI for content generation — plain-language summaries, registry authoring, and even protocol development, which indirectly influences disclosure quality. There's also interest in using AI to interpret regulatory requirements.
“But I'll be honest,” she continues, “the technology isn't reliable enough yet to operate without human oversight. AI-assisted writing is improving quickly, but you absolutely need someone reviewing the output to catch errors or nonsensical content. It's a powerful tool, but it requires expert judgment to use effectively.”
 David Wild
Senior Reporter at In Vivo
Citeline
David Wild
Senior Reporter at In Vivo
Citeline
David Wild, Senior Reporter at Citeline's In Vivo, says, “We're moving past the potential of AI and skepticism into actual data and partnerships, with companies beginning to show real results in drug discovery and start-ups locking in deals by building highly specialized datasets for drug discovery.
“The next wave of AI includes virtual cells and digital twins that will, with increasing accuracy, mimic individual patient biology, along with federated learning initiatives that are breaking down data silos to create larger, more useful datasets. AI-based trial optimization is gaining traction with the promise of reducing patient recruitment numbers, accelerating recruitment, and cutting failure rates. However, given the long drug development timelines, it will still take time to see if these tools truly deliver more effective drugs faster and cheaper.”
While Chmielewska agrees that AI is important in R&D, she emphasizes that data quality is integral for AI systems and integration to flourish.

Darcy Grabenstein
Director of Content Strategy and Thought Leadership | Citeline
Darcy is the Director of Content Strategy and Thought Leadership for Citeline. A journalist by training, she has more than 30 years of experience in marketing, advertising, and public relations.
How will patient recruitment evolve in 2026?
Recruitment will increasingly leverage AI and real-world data (RWD) for comprehensive patient matching, including tokenization to locate hard-to-find patients.
How will regulatory changes impact clinical trials in 2026?
The updated ICH GCP E6(R3) guideline emphasizes risk-proportionate, data-driven, tech-enabled trials with strong governance. Additionally, the UK Medicines for Human Use (Clinical Trials) Amendment Regulations 2025 will take effect in April 2026, reinforcing ethical frameworks and transparency requirements. ISRCTN may become the preferred registry for international clinical trials.
What role will AI play in clinical development?
AI will reshape protocol design, patient recruitment, and trial optimization. Formal AI governance and cross-functional data/AI teams will become standard, ensuring accountability and compliance with regulatory expectations.




To combat clinical trial attrition, sponsors must recruit the right-fit patients from the start, then employ retention measures to ensure patients remain comfortable and confident throughout the trial.
To enable the booking feature, please enable all cookies in your browser.

